During the COVID-19 pandemic, older people were labelled as vulnerable and dispensable overnight
Because ageism is bad for health.
During the COVID-19 pandemic, older people were labelled as vulnerable and dispensable overnight – a direct effect on mortality related to age was obviously associated with access to treatment.
The Australian Royal Commission into Aged Care Quality and Safety also outlines numerous issues and areas for improvement (tinyurl.com/AgedCareReport). Further, the ABC has nicely summarised issues of ageism that are broader than residential care (tinyurl.com/ABCageism).
Those people who feel discriminated against (high age discrimination on questionnaires) have worse diseases and incur more costs. Using population prevalence estimates, and adjusting for confounders, one study found that one year of ageism costs US$63 billion, or one of every seven dollars spent on eight common chronic diseases.1
Potentially, those subjected to discrimination don’t value themselves, don’t look after their health and are denied opportunities (sounds familiar!). Impacts on loneliness, social isolation and even cognition have been associated with ageism against older people.
A systematic review published last year found the simultaneous impact of structural ageism, where institutions reinforce systematic bias against older people, and individual ageism, where older people assimilate negative views of ageing from their culture, results in worse health outcomes all around the world and across age groups, and has greater negative impact on people otherwise economically and educationally disadvantaged.2
This review reported on 50 studies about physical illness and 42 studies about mental illness where ageism was associated with worse outcomes. On a brighter note, when older people resisted negative age stereotypes, they were less likely to experience suicidal ideation, post-traumatic stress disorder and anxiety.2
Mechanisms by which ageism impacts on health include psychological (low self-efficacy, less perceived control, lack of purpose in life, greater intention to leave work), behavioural (less physical activity, less career-advancing activities) and physiological (C-reactive protein partially mediates the relationship between positive self-perceptions of ageing and longevity) pathways.2
There are examples of successful interventions that changed attitudes towards older people, knowledge about ageing and comfort with older people.
Combined interventions with education and intergenerational contact worked the best, and the most impacted were women, and adolescent and young adult groups. However, no significant effects on anxiety about one’s own ageing or interest in working with older adults were found.3
Whether health outcomes for older people were improved was not studied – this would be hard to study as the impacts of ageism are likely to be accrued over a lifetime.3
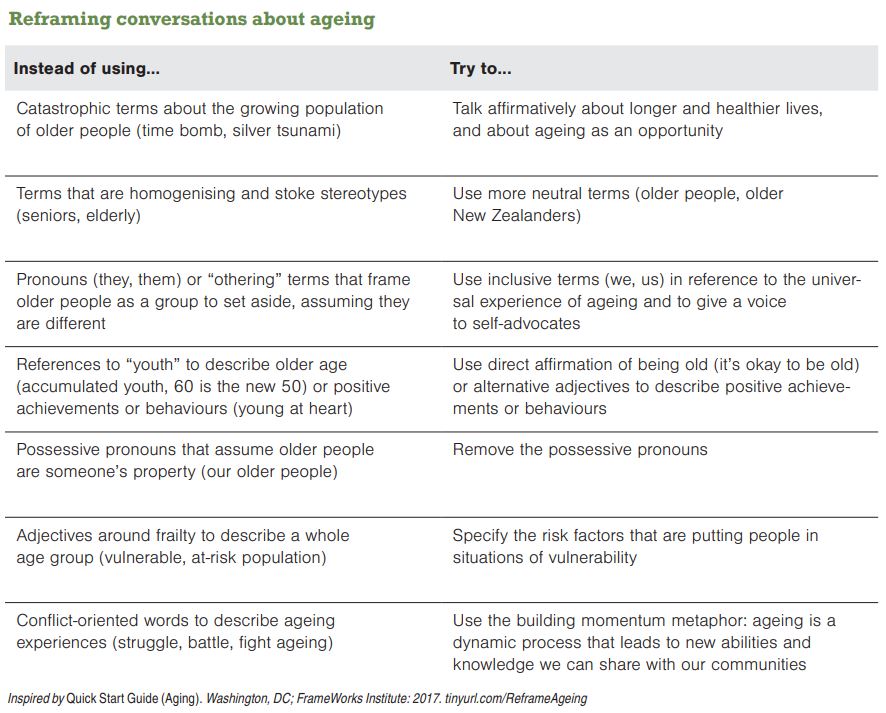
So, I invite you to the bandwagon of anti-ageism, to think about older people positively, to act positively and encourage full participation in society for your older patients. Their health will benefit, and your job will be easier as a result.




![New Zealand Doctor Rata Aotearoa editor Barbara Fountain, RNZCGP president elect and Tauranga-based specialist GP Luke Bradford, Ministry of Health clinical chief advisor rural health Helen MacGregor, and Health New Zealand Te Whatu Ora clinical director primary and community care Sarah Clarke [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/1.%20Barbara%20Fountain%2C%20Luke%20Bradford%2C%20Helen%20MacGregor%20and%20Sarah%20Clarke.jpg?itok=091NETXI)
![Ngāti Porou Oranga specialist GP Elina Pekansaari and Te Nikau Hospital specialist in general practice and rural hospital medicine David Short [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/2.%20Elina%20Pekansaari%20and%20David%20Short.jpg?itok=h5XfSBVM)
![Locum specialist GP Margriet Dijkstra and OmniHealth regional operations manager (southern) Patricia Morais-Ross [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/3.%20Margriet%20Dijkstra%20and%20Patricia%20Morais-Ross.jpg?itok=jkrtRfJC)
![Golden Bay dairy farmer and dairy industry health and safety doctoral student Deborah Rhodes, and Golden Bay Community Health specialist GP Rachael Cowie [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/4.%20Deborah%20Rhodes%20and%20Rachael%20Cowie.jpg?itok=oM0_GcJc)
![Hauora Taiwhenua clinical director rural health Jeremy Webber, Australian College of Rural and Remote Medicine president Rod Martin and Observa Care director of business operations Deborah Martin, the wife of Dr Martin [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/5.%20Jeremy%20Webber%2C%20Rod%20Martin%20and%20Deborah%20Martin%2C%20the%20wife%20of%20Dr%20Martin.jpg?itok=P_aGmX_H)
![Spark Health chief executive John Macaskill-Smith and client director Bryan Bunz [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/6.%20John%20Macaskill-Smith%20and%20Bryan%20Bunz.jpg?itok=5yJvVZ0I)
![Associate dean (rural) Kyle Eggleton, third-year medical student Roselle Winter, and second-year pharmacy student Alina Khanal, all from the University of Auckland [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/7.%20Kyle%20Eggleton%2C%20Roselle%20Winter%20and%20Alina%20Khanal.jpg?itok=RQLd3TEs)
![Health New Zealand Te Whatu Ora clinical editor and specialist in general practice and rural hospital medicine Anu Shinnamon, and Whakarongorau chief clinical officer Ruth Large [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/8.%20Anu%20Shinnamon%20and%20Ruth%20Large.jpg?itok=i5TMswY9)
![Te Kahu Hauora Practice specialist GP Jane Laver and Ngāti Kahungunu ki Tāmaki-nui-a-Rua chief operations manager Tania Chamberlain [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/9.%20Jane%20Laver%20and%20Tania%20Chamberlain.jpg?itok=jtMklaCZ)