What to ask
When interpreting liver enzyme test results, common questions to ask are:
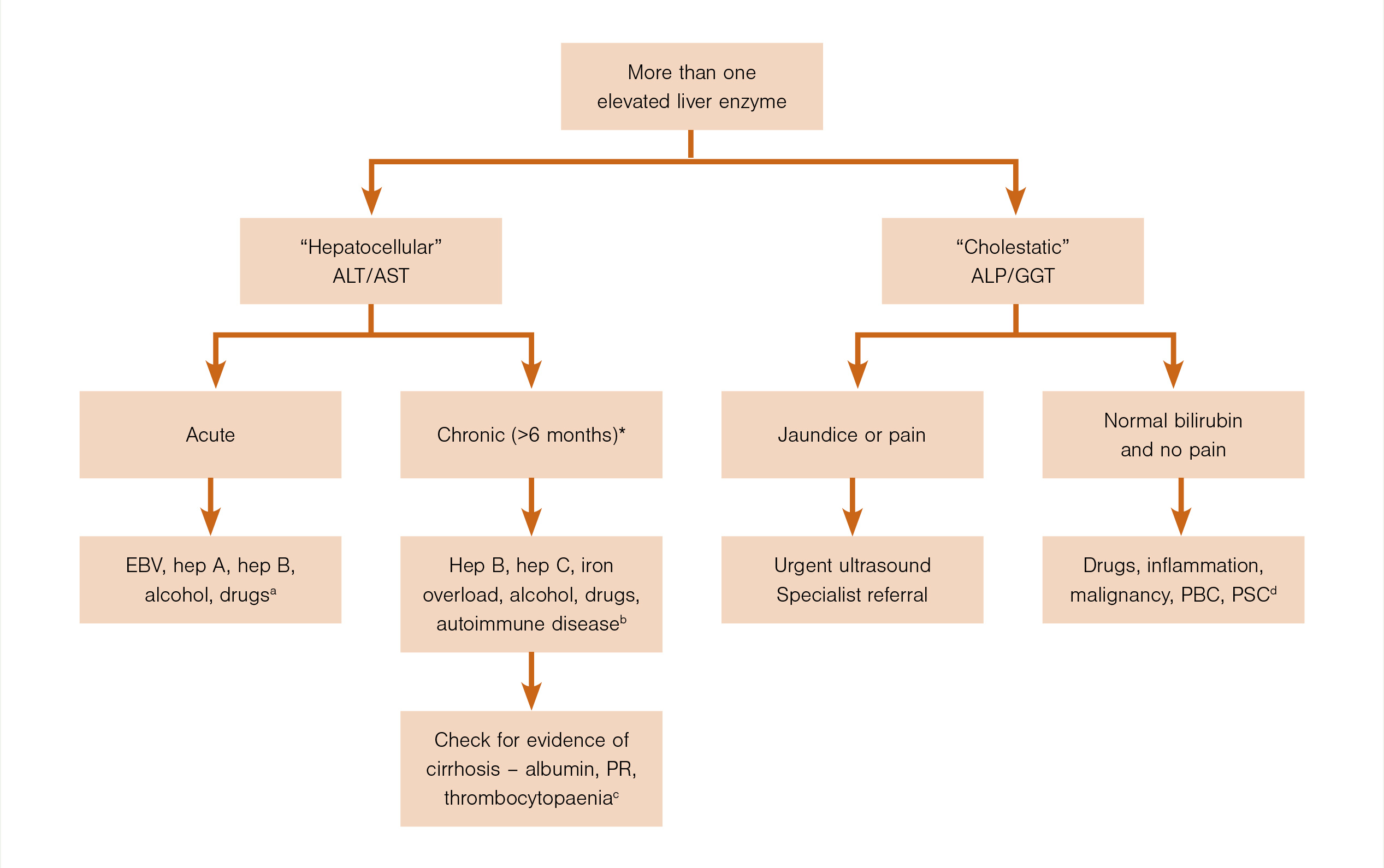
1. Is the pattern “hepatocellular” (mainly ALT/AST elevation) or is it “cholestatic” (mainly alkaline phosphatase [ALP] and GGT elevation)?
- If it is mainly hepatocellular, refer to question 2 below.
- If it is a mixture of both “patterns”, the predominant problem is usually obvious.
- In chronic hepatitis, mild cholestasis is common, but the pattern is predominantly hepatocellular.
- In acute biliary obstruction, ALT/AST levels may rise during the first two to three days (in addition to the cholestatic picture) but return to near normal if obstruction persists. Note that acute obstruction is usually associated with “biliary-type” pain.
- Biliary-type pain with cholestatic liver enzymes requires urgent specialist review even if an ultrasound is normal. The most likely cause is stones in the common bile duct. Magnetic resonance cholangiography may be required if there is diagnostic uncertainty.
- Reasons for a cholestatic pattern with no pain or jaundice are covered in a later section.
2. Is there evidence of persistent elevation of ALT/AST levels over more than one to two months?
- More than six months of elevated ALT/AST levels defines chronic hepatitis.
- In practical terms, chronic hepatitis should be considered from the onset and becomes more likely if there are persistent abnormalities after one to two months.
- Many patients with newly discovered elevation of ALT/AST will prove to have chronic liver disease.
- If the initial level of ALT/AST is greater than 500IU/L, it is most likely to be acute hepatitis/liver injury.
Tests for acute hepatitis
A diagnosis of alcohol-related liver disease rests primarily on the patient’s history and a high index of suspicion, rather than the pattern of liver enzyme test results
Acute hepatitis is usually associated with symptoms of an “acute illness”.
The main tests for acute viral hepatitis are hepatitis A immunoglobulin M and hepatitis B surface antigen, and tests for cytomegalovirus (<2 per cent of acute viral hepatitis cases) and Epstein–Barr virus (50 per cent) – the most common cause of acutely elevated ALT/AST levels in the community is infectious mononucleosis.
Hepatitis C does cause acute hepatitis but is almost always asymptomatic, and hepatitis D only occurs in the presence of hepatitis B infection.
Consider drugs as a cause of acute hepatitis. These can include phenytoin, isoniazid, diclofenac, allopurinol andazathioprine. Your patient may also have rash, fever and eosinophilia.
Also consider alcohol-induced liver disease. This may cause “hepatitis”, with AST and ALT levels that are relatively low for acute hepatitis (100–300IU/L). Look for elevated GGT (100–300IU/L) but normal ALP levels, macrocytosis, an AST level greater than ALT (a ratio >2.0 is very suggestive of alcohol-induced liver disease), elevated white blood cell count and fever if the hepatitis is more severe. A diagnosis of alcohol-related liver disease rests primarily on the patient’s history and a high index of suspicion, rather than the pattern of liver enzyme test results.
Rarely does autoimmune hepatitis present as an acute illness, and even rarer is Wilson disease. The latter can be considered if the patient is aged less than 40 – check serum copper and caeruloplasmin.
Paracetamol overdose will elevate the ALT level to over 1000IU/L. Check the INR. Most patients will need emergency department review.
Massive elevations in the ALT level are only seen in hospital settings and are predominantly due to cardiogenic shock and ischaemic hepatitis.
Acute hepatic vein obstruction can occur, particularly in the setting of haematological malignancy.
Tests for chronic hepatitis
In chronic hepatitis, the ALT level is usually only 1.5–3 times the upper limit of normal. If ALT levels have been elevated for more than one to two months, order the relevant tests – request hepatitis B surface antigen, hepatitis C antibodies (if positive, follow with hepatitis C PCR), autoantibodies (ANA and SMA), serum ferritin and iron studies (iron and total iron-binding capacity).
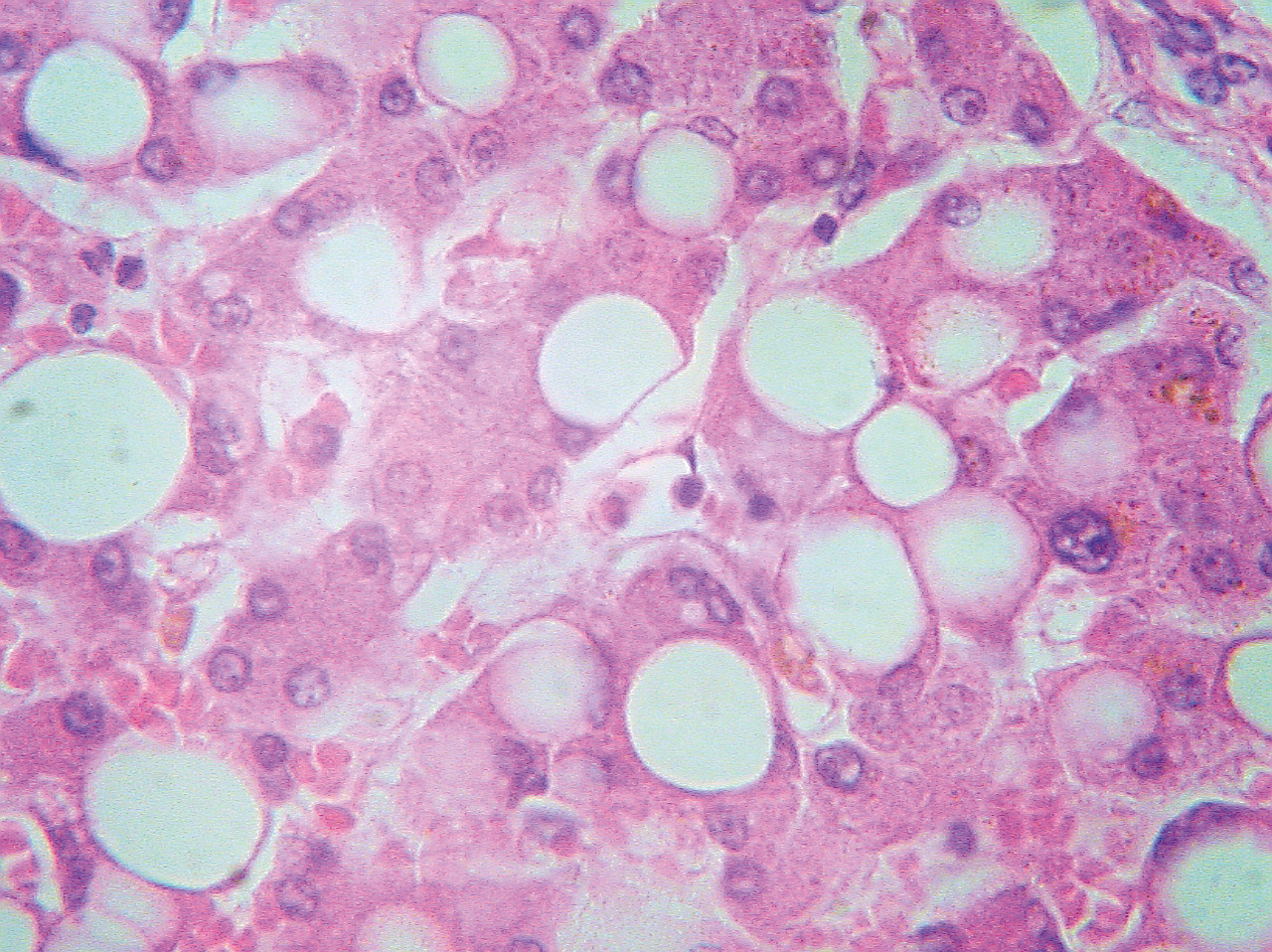
The most common cause of raised ALT/AST levels is fatty liver. This is usually combined with a mild elevation of GGT.
Raised serum ferritin may be due to haemochromatosis but also occurs with liver inflammation (it is common with fatty liver and excess alcohol consumption). Request liver ultrasound and evaluate risk factors for fatty liver. If iron saturation is high (>50 per cent) or ferritin is greater than 750μg/L, order a gene test for haemochromatosis (C282Y mutation in the HFE gene).
As in acute hepatitis, consider drugs. Any drug can be associated with chronic hepatitis – isoniazid, nitrofurantoin, ketoconazole, NSAIDs. Also consider illicit drugs, anabolic steroids and herbal treatments.
Autoimmune hepatitis is associated with raised serum globulins (often over two times the normal level); check autoantibodies (ANA and SMA).
Check the alpha-fetoprotein level (elevated in primary hepatocellular cancer), particularly if there is suspicion of cirrhosis.
The ratio of AST to ALT is often discussed with reference to a diagnosis of alcohol-related liver disease. An AST:ALT ratio of 2:1 is suggestive, but this is seen in only 50 per cent of cases. Clinical suspicion and careful questioning are more important.
Check for evidence of cirrhosis
Impairment of hepatic function or portal hypertension indicate cirrhosis. It is important to look for impairment in all patients with chronic hepatitis.
Check the serum albumin level and prothrombin ratio. Even borderline abnormal results are likely to be significant in the setting of chronic hepatitis. Albumin is a plasma protein exclusively synthesised by the liver with a circulating half-life of three weeks. A reduction in serum albumin usually indicates liver disease of more than three weeks’ duration, although any significant illness can decrease albumin levels because of cytokine effects.
Thrombocytopaenia suggests portal hypertension. An enlarged spleen may be detected by ultrasound.
‘Cholestatic’ pattern, no pain or jaundice
Ultrasound is the key test when elevated liver enzymes show a cholestatic pattern with no pain or jaundice.
Cholestasis may be a non-specific feature of disseminated cancer. Metastatic disease of the liver usually has a mixed pattern, with only mild elevation of ALP and GGT levels. It is usually confirmed by ultrasound. If bile ducts are dilated and there is no biliary-type pain, the cause is likely to be malignant bile duct obstruction.
If the ultrasound is normal, several reasons for a cholestatic pattern need to be reviewed:
- Consider drugs.
- Phenothiazines – your patient can continue these if there is mild cholestasis (two to three times normal values for ALP and GGT). Remember that prochlorperazine (Stemetil) may cause cholestasis.
- Amoxicillin + clavulanic acid (Augmentin) and flucloxacillin – may cause a progressive cholestasis with slow resolution over several months after the drug is discontinued.
- Erythromycin – may present with acute right upper quadrant pain.
- Non-specific cholestasis is common with sepsis and in chronic inflammatory conditions (eg, inflammatory bowel disease).
- Mild elevation (mixed pattern) is common with predominant right-sided heart failure related to hepatic congestion.
- If cholestasis is chronic (more than three to six months) and progressive, consider chronic liver disorders, such as primary biliary cirrhosis and sclerosing cholangitis, and HIV cholangiopathy. Order anti-mitochondrial antibody. Specialist referral is required for magnetic resonance cholangiopancreatography with or without liver biopsy.
Asymptomatic benign liver lesions (usually haemangiomas) are common and are not associated with liver enzyme abnormalities.
Drugs and monitoring of liver enzymes
A definite benefit from regular monitoring of liver enzyme tests is evident in only a few examples:
- Isoniazid – only a transient elevation in liver enzymes is usual, but isoniazid must stop if a progressive rise is evident. Fulminant hepatitis may occur – the risk is higher if the patient’s age is over 50.
- Methotrexate – early elevation of ALT/AST levels can occur in the first few months after initiation, but this may not be important. Progressive changes may suggest hepatic fibrosis and need for further evaluation with a FibroScan.
- Azathioprine – hepatitis may occur in the first few months after initiation and require cessation of drug; 6-mercaptopurine may be a useful alternative.
- Statins – mild elevations of ALT are common, particularly in the first few months after beginning treatment, and usually related to underlying fatty liver (there may be shifts in intrahepatic lipids during initial treatment).
Role of liver biopsy
When investigating abnormal liver enzyme tests, the majority of diagnoses are made by undertaking a patient history (with a careful review of drug history), physical examination and blood tests. A FibroScan can diagnose or exclude advanced liver disease. Only a few patients will require a liver biopsy.
General considerations
Always ask about medication – prescribed and over the counter. Common agents that may cause a rise in liver enzymes are antibiotics, antiepileptics, NSAIDs and herbal products.
Rare and surprising causes of raised liver function test results are coeliac disease and both hypothyroidism and hyperthyroidism. Abnormal liver function tests in late pregnancy are often important and may need urgent review.
Should the diagnosis remain unclear in the presence of abnormal liver function test results:
- discontinue hepatotoxic drugs
- discontinue alcohol
- assess again for fatty liver and risk factors.
Read more in “Liver function tests in primary care” on the BPACnz website (bpac.org.nz/2022/LFTs.aspx).







![New Zealand Doctor Rata Aotearoa editor Barbara Fountain, RNZCGP president elect and Tauranga-based specialist GP Luke Bradford, Ministry of Health clinical chief advisor rural health Helen MacGregor, and Health New Zealand Te Whatu Ora clinical director primary and community care Sarah Clarke [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/1.%20Barbara%20Fountain%2C%20Luke%20Bradford%2C%20Helen%20MacGregor%20and%20Sarah%20Clarke.jpg?itok=091NETXI)
![Ngāti Porou Oranga specialist GP Elina Pekansaari and Te Nikau Hospital specialist in general practice and rural hospital medicine David Short [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/2.%20Elina%20Pekansaari%20and%20David%20Short.jpg?itok=h5XfSBVM)
![Locum specialist GP Margriet Dijkstra and OmniHealth regional operations manager (southern) Patricia Morais-Ross [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/3.%20Margriet%20Dijkstra%20and%20Patricia%20Morais-Ross.jpg?itok=jkrtRfJC)
![Golden Bay dairy farmer and dairy industry health and safety doctoral student Deborah Rhodes, and Golden Bay Community Health specialist GP Rachael Cowie [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/4.%20Deborah%20Rhodes%20and%20Rachael%20Cowie.jpg?itok=oM0_GcJc)
![Hauora Taiwhenua clinical director rural health Jeremy Webber, Australian College of Rural and Remote Medicine president Rod Martin and Observa Care director of business operations Deborah Martin, the wife of Dr Martin [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/5.%20Jeremy%20Webber%2C%20Rod%20Martin%20and%20Deborah%20Martin%2C%20the%20wife%20of%20Dr%20Martin.jpg?itok=P_aGmX_H)
![Spark Health chief executive John Macaskill-Smith and client director Bryan Bunz [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/6.%20John%20Macaskill-Smith%20and%20Bryan%20Bunz.jpg?itok=5yJvVZ0I)
![Associate dean (rural) Kyle Eggleton, third-year medical student Roselle Winter, and second-year pharmacy student Alina Khanal, all from the University of Auckland [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/7.%20Kyle%20Eggleton%2C%20Roselle%20Winter%20and%20Alina%20Khanal.jpg?itok=RQLd3TEs)
![Health New Zealand Te Whatu Ora clinical editor and specialist in general practice and rural hospital medicine Anu Shinnamon, and Whakarongorau chief clinical officer Ruth Large [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/8.%20Anu%20Shinnamon%20and%20Ruth%20Large.jpg?itok=i5TMswY9)
![Te Kahu Hauora Practice specialist GP Jane Laver and Ngāti Kahungunu ki Tāmaki-nui-a-Rua chief operations manager Tania Chamberlain [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/9.%20Jane%20Laver%20and%20Tania%20Chamberlain.jpg?itok=jtMklaCZ)