So, I decided to go through the more detailed data spreadsheets available online. However, the data Mr Brown’s media statement is based on is not yet available, which meant I couldn’t look at whether the good news was good news for everyone when broken down by ethnicity or relative deprivation.
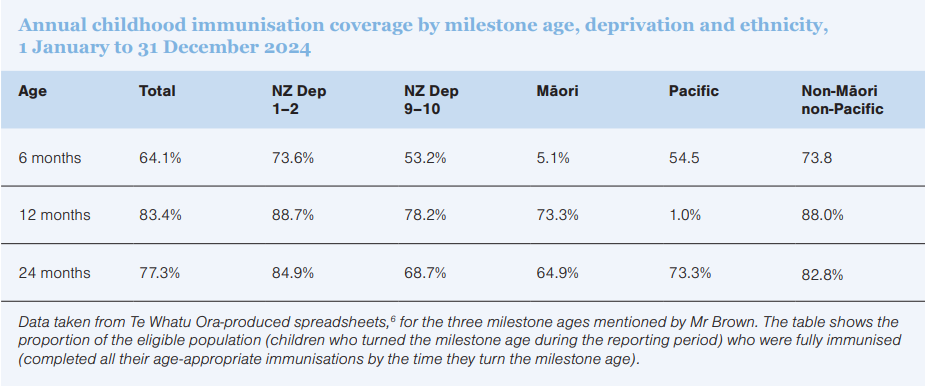
Instead, I looked at the annual childhood immunisation coverage by age, district, region, deprivation and ethnicity as of December 2024. This period is the most up-to-date data on the Health New Zealand Te Whatu Ora website,5 but I stress that this is not the data the media statement was based on. There are some clear patterns in this data, which might be best seen in the table below.
What is striking in this data is the way those who are the most materially well-off (NZ Dep 1-2) and non-Māori non-Pacific ethnic groups have the highest immunisation proportion of eligible children immunised, and these proportions are very similar. They are also higher than the total population figures.
Equally striking is that Māori children are the least likely to be fully immunised at every milestone age. Only 45.1 per cent of the youngest Māori pēpi are fully immunised at six months old, which is incidentally slightly worse than in December 2023 (46.9 per cent).
There is no additional statistical analysis from me here, policy rather than maths being my area of expertise, so there could be even more to the picture to understand. But, nevertheless, I think this table makes the point that total population isn’t telling us the whole story
Perhaps it is a bit much to expect a ministerial media statement to include a proper analysis of system performance.
Certainly, nuance isn’t easily communicated in 300 words. But in an area that is infamous for its inequities and so closely connected to outcomes for tamariki Māori, it is still reasonable to expect any good news to be subject to scrutiny.
I look forward to seeing the more detailed data tables from Te Whatu Ora to see how the story goes – beyond the total population headline.







![New Zealand Doctor Rata Aotearoa editor Barbara Fountain, RNZCGP president elect and Tauranga-based specialist GP Luke Bradford, Ministry of Health clinical chief advisor rural health Helen MacGregor, and Health New Zealand Te Whatu Ora clinical director primary and community care Sarah Clarke [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/1.%20Barbara%20Fountain%2C%20Luke%20Bradford%2C%20Helen%20MacGregor%20and%20Sarah%20Clarke.jpg?itok=091NETXI)
![Ngāti Porou Oranga specialist GP Elina Pekansaari and Te Nikau Hospital specialist in general practice and rural hospital medicine David Short [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/2.%20Elina%20Pekansaari%20and%20David%20Short.jpg?itok=h5XfSBVM)
![Locum specialist GP Margriet Dijkstra and OmniHealth regional operations manager (southern) Patricia Morais-Ross [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/3.%20Margriet%20Dijkstra%20and%20Patricia%20Morais-Ross.jpg?itok=jkrtRfJC)
![Golden Bay dairy farmer and dairy industry health and safety doctoral student Deborah Rhodes, and Golden Bay Community Health specialist GP Rachael Cowie [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/4.%20Deborah%20Rhodes%20and%20Rachael%20Cowie.jpg?itok=oM0_GcJc)
![Hauora Taiwhenua clinical director rural health Jeremy Webber, Australian College of Rural and Remote Medicine president Rod Martin and Observa Care director of business operations Deborah Martin, the wife of Dr Martin [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/5.%20Jeremy%20Webber%2C%20Rod%20Martin%20and%20Deborah%20Martin%2C%20the%20wife%20of%20Dr%20Martin.jpg?itok=P_aGmX_H)
![Spark Health chief executive John Macaskill-Smith and client director Bryan Bunz [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/6.%20John%20Macaskill-Smith%20and%20Bryan%20Bunz.jpg?itok=5yJvVZ0I)
![Associate dean (rural) Kyle Eggleton, third-year medical student Roselle Winter, and second-year pharmacy student Alina Khanal, all from the University of Auckland [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/7.%20Kyle%20Eggleton%2C%20Roselle%20Winter%20and%20Alina%20Khanal.jpg?itok=RQLd3TEs)
![Health New Zealand Te Whatu Ora clinical editor and specialist in general practice and rural hospital medicine Anu Shinnamon, and Whakarongorau chief clinical officer Ruth Large [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/8.%20Anu%20Shinnamon%20and%20Ruth%20Large.jpg?itok=i5TMswY9)
![Te Kahu Hauora Practice specialist GP Jane Laver and Ngāti Kahungunu ki Tāmaki-nui-a-Rua chief operations manager Tania Chamberlain [Image: NZD]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-05/9.%20Jane%20Laver%20and%20Tania%20Chamberlain.jpg?itok=jtMklaCZ)